
TEOAEs Test Procedures


- Details
- Parent Category: Basics of OAEs
- Category: TEOAEs
- Last Updated on Saturday, 29 December 2012 15:16
- Hits: 24300
Editor's Note:A portion of the material presented in the TEOAE pages has appeared in the NATASHA (Network and Tools for the Assessment of Speech/Language and Hearing Ability) project web pages.
Equipment and Stimuli for human measurements
a) Set-up (equipment, test environment, etc.):
For measuring the TEOAEs the ILO-92, ILO-292, (Otodynamics) and Celesta / Capella (Madsen) standard equipment are used in most cases.
Editor's Note: This situation is bound to change very soon as the Otodynamics TEOAE patent has expired , and new equipment will enter the market as soon as in the second quarter of 2001.
The ear canal is closed with a probe and a cuff. The probe is connected to a loudspeaker and a microphone.
By default the stimuli are trains of 4 biphasic clicks of 80 ms in the non-linear position (+1 +1 +1 -3). The stimulus intensity is set at 84 dB peak equivalent SPL (0.3 Pa peak) with the spectrum adjusted as flat as possible (band pass filter of 500-6000 Hz). The window for the TEOAE recording is set at 20.49 ms, but in order to ensure a significant stimulus artifact rejection the first 2.5 ms of the recording are suppressed.
Due to recent advances in the TEOAE technology it is now possible to use a shorter recording window (12.5 ms) with a protocol called QuickScreen. A number of studies have also indicated that it is possible to use a Linearprotocol (of 70 - 75 dB SPL) to reliably record neonatal and adult subject responses.


Another type of TEOAE stimuli, but not commonly used, are the tone pips or tone-bursts. It is possible to elicit TEOAE responses using modulated tone-pips of a 4ms duration at frequencies of 1.0, 2.0 and 4.0 kHz, but the first 4-6 ms of the TEOAE response are contaminated by the stimulus artifact. In terms of clinical uses it is obvious that responses evoked by tone-pips have a significant clinical advantage over the use of clicks alone. In addition, a recent study by Vinck et al (1998) has reported that a correct classification of pure-tone thresholds between 500 and 4000 Hz up to 100% was possible, when variables from click and tone-burst otoacoustic measurements were used . An interesting aspect of the tone-pip TEOAE generation is the possibility to calculate the OAE latency. The OAE latency is impossible to compute in the click-evoked TEOAEs, due to the presence of numerous frequency components (the latter can be overcome by using a wavelet transform decomposing the original TEOAE response into a set of specific components. For more info see Methods of TEOAE signal analysis). The TEOAE latency is a very good distriminant variable between normal and hearing impaired ears, and it is relatively easy to build reference templates to employ in the identification of the hearing status of an adult or neonatal subject (for more information on how to build these reference templates you might consult Hatzopoulos et al, Audiology, 1995; Hatzopoulos et al, Audiology-Neurotology, 1998)
The reader who is interested in tone-pip, tone-burst stimuli might consult the following papers(the titles are MEDLINE enabled, and by clicking on the authors names you might access the paper's abstract):
Smurzynski J, Probst R.
- Intensity discrimination, temporal integration and gap detection by normally-hearing subjects with weak and strong otoacoustic emissions. Audiology. 1999 Sep-Oct;38(5):251-6.
Harrison WA, Norton SJ.
- Characteristics of transient evoked otoacoustic emissions in normal-hearing and hearing-impaired children. Ear Hear. 1999 Feb;20(1):75-86.
Vinck BM, Van Cauwenberge PB, Corthals P, De Vel E.
- Multi-variant analysis of otoacoustic emissions and estimation of hearing thresholds: transient evoked otoacoustic emissions. Audiology. 1998 Nov-Dec;37(6):315-34.
O-Uchi T, Kanzaki J, Ogata A, Inoue T, Mashino H, Yoshihara S, Satoh Y.
- Pathophysiology of hearing impairment in acoustic neuroma with profound deafness: analysis by evoked otoacoustic emission and promontory stimulation test. Acta Otolaryngol Suppl. 1994;514:95-100.
O-Uchi T, Kanzaki J, Satoh Y, Yoshihara S, Ogata A, Inoue Y, Mashino H.
- Age-related changes in evoked otoacoustic emission in normal-hearing ears. Acta Otolaryngol Suppl. 1994;514:89-94.
Hauser R, Probst R, Harris FP.
- Effects of atmospheric pressure variation on spontaneous, transiently evoked, and distortion product otoacoustic emissions in normal human ears. Hear Res. 1993 Sep;69(1-2):133-45.
Hauser R, Probst R, Lohle E.
- Click- and tone-burst-evoked otoacoustic emissions in normally hearing ears and in ears with high-frequency sensorineural hearing loss. Eur Arch Otorhinolaryngol. 1991;248(6):345-52.
TEst Procedures
When the user has selected the type of TEOAE protocol (QuickScreen, nonlinear or linear) may proceed to the acquisition of the TEOAE response. The protocol below refers to the procedural steps using the ILO88.
- Insert the acoustic probe, fitted with a disposable plastic tip, into the patient's ear.
- A standard click stimulus is applied and the sound in the ear canal is displayed as a waveform and spectrum so that the operator can adjust the fit of the probe and ensure proper stimulation for performing correctly the test. The cable of the probe should be directed 45° towards the top of the head. Experience has shown that this angle is not feasible with neonatal subjects, where a wider angle is used. The position of the probe into the external auditory canal is a crucial component of the proper conduction of the test especially in neonatal subjects. An example of an ideal stimulus-response is shown in Figure 1below.
-
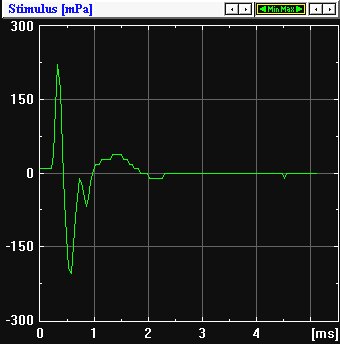 Figure 1: Ideal shape of a click TEOAE stimulus
Figure 1: Ideal shape of a click TEOAE stimulusAn erroneous probe position may effect the lower TEOAE frequencies due to a bad coupling between the probe body and the external auditory canal. But in no case an erroneous position of a probe can result in absence of response, with the exception when the probe is completely out of the external auditory meatus. These considerations are valid ONLYfor the TEOAEs and cannot be extrapolated for the DPOAEs.
Figure 2: Response from an agitated neonatal subject. The stimulus profile indicates that due to the movements of the subject, the probe is not placed in an optimal position. Nevertheless the obtained response is a PASS.
- Following the check-fit, the test may start. The preset stimulus is repeated as many as 256 times (1024 clicks in total) and the "delayed" cochlear responses in the ear canal are acquired and accumulated in a memory bank in order to enhance the detection of the small cochlear signals against the background noise. It should be noted that neonatal subjects have significantly strongeremissions than adults and under normal conditions (the subject is calm) an average of 20 stimuli (80 clicks) can be sufficient.
The patient (adults and children) should be quiet and sitting comfortably and still. Infants, if possible, should be lying still.
- The stop-criteria for the test vary. The majority of programs use a pre-specified number of sweeps for each subject category (neonates, NICU residents, children, young adults, adults). It is also common to stop the recording when a variable reaches a specific value: For example when the overall reproducibility exceeds 75% or when the S/N ratio at certain frequencies is above a pre-determined level. NOTE:These criteria, independently how stringent might be, cannot guarantee that the employed OAE procedure will yield excellent results in the identification of both normal and hearing impaired ears. Signal theory indicates that by increasing the sensitivity of a test procedure the specificity decreases and vice versa. Today a sensitivity of 90 - 95 % is well accepted.
The reader who is interested in more information on the TEOAE evaluation criteria (sometimes termed also as scoring criteria) might consult the following papers (the titles are MEDLINE enabled, and by clicking on the authors names you might access the paper's abstract):
Norton SJ, Gorga MP, Widen JE, Folsom RC, Sininger Y, Cone-Wesson B, Vohr BR, Mascher K, Fletcher K.
- Identification of neonatal hearing impairment: evaluation of transient evoked otoacoustic emission, distortion product otoacoustic emission, and auditory brain stem response test performance. Ear Hear. 2000 Oct;21(5):508-28.
Norton SJ, Gorga MP, Widen JE, Vohr BR, Folsom RC, Sininger YS, Cone-Wesson B, Fletcher KA.
- Identification of neonatal hearing impairment: transient evoked otoacoustic emissions during the perinatal period. Ear Hear. 2000 Oct;21(5):425-42.
Hatzopoulos S, Tsakanikos M, Grzanka A, Ratynska J, Martini A.
- Comparison of neonatal transient evoked otoacoustic emission responses recorded with linear and QuickScreen protocols. Audiology. 2000 Mar-Apr;39(2):70-9. PMID: 10882045
Aidan D, Avan P, Bonfils P.
- Auditory screening in neonates by means of transient evoked otoacoustic emissions: a report of 2,842 recordings. Ann Otol Rhinol Laryngol. 1999 Jun;108(6):525-31.
Rhodes MC, Margolis RH, Hirsch JE, Napp AP.
- Hearing screening in the newborn intensive care nursery: comparison of methods. Otolaryngol Head Neck Surg. 1999 Jun;120(6):799-808.
Gorga MP, Neely ST, Bergman BM, Beauchaine KL, Kaminski JR, Peters J, Schulte L, Jesteadt W.
- A comparison of transient-evoked and distortion product otoacoustic emissions in normal-hearing and hearing-impaired subjects. J Acoust Soc Am. 1993 Nov;94(5):2639-48.