Effects of Mobile Telephone's Electromagnetic Field on Hearing
By Orhan Ozturan, Tamer Erdem, Murat Cem Miman,
Mahmut Tayyar Kalcioglu, Semih Oncel
Inonu University,
School of Medicine, Otorhinolaryngology Department
Malatya, Turkey
orhanent@yahoo.com
Phone Int + , Fax Int +
Article originally published in ACTA-LARYNGOLOGICA (April 2002)
Introduction The use of mobile telephones is rapidly increasing world-wide. They transmit and receive microwave radiation at frequencies of about 900 Megahertz (MHz) and 1800 MHz and these frequencies excite the rotations of the water and some organic molecules and have been attributed to thermal and non-thermal effects. The widespread use of mobile telephones has given rise to the question of whether the EMFs created by mobile telephones is detrimental to the hearing of their users.
Mobile telephone use necessitates to hold in close proximity with the ear, and so far it has not been reported as a cause of hearing loss in the literature. If it causes subtle cochlear deleterious effects, these may be observable through changes in evoked otoacoustic emissions (OAEs). The present study was designed to search for the acute after-effect of mobile telephone EMF on human hearing measured by changes in evoked OAEs.
Subjects and Methods
Thirty normal-hearing adults (17 males and 13 females) between the ages of 19 and 36 years (mean age 25 years) volunteered to participate in this study. Only the right ear was exposed to EMF and evaluated in this study. After confirming the subject's health status with a complete medical and otologic history, and otoscopic examination, tympanometry was performed to eliminate the possibility of middle ear problems. The criteria for normal hearing were that the pure-tone thresholds be at 20-dB HL or better for the octave frequencies (250-8000 Hz) and for the interoctave frequencies (1500, 3000 and 6000 Hz), and that tympanometry showed normal middle ear function. Volunteers meeting these criteria for normal hearing were enrolled to the study for evoked OAE testing sessions.
The mobile telephone utilized in this study was the Panasonic GD 600. This mobile telephone transmits and receives radio signals in the 900 MHz range using the GSM system. In spite of repeated inquires to the manufacturer about its SAR level, the manufacturer never responded.
For the purposes of monitoring the potential negative effects of EMFs from a mobile telephone on hearing, transiently-evoked (TEOAEs) and distortion-product (DPOAEs) OAEs were recorded consecutively and analyzed utilizing ILO-96 cochlear emission analyzer (Otodynamics, London, United Kingdom). Four evoked OAE test sessions were performed separately for each subject. The baseline measurement was repeated 10 minutes after completion of the test to confirm test/retest reliability. After the second measurement, the subjects held the activated mobile telephone on their right ear for 10 minutes without interruption in the room next to the sound-treated testing room.
The subject did not converse with anyone during this time to avoid the potentiality of the negative acoustic effect on the outer hair cells for the purpose of being under the influence of the mobile telephone EMF only. The third measurement was performed immediately after the 10-minute telephone use. Finally, a fourth measurement was carried out 10 minutes after the last testing for the recovery of the hearing, in case there was any alteration due to EMF exposure. Each evoked OAE measurement session lasted for about 2 to 2.5 minutes.
The Transiently-evoked OAEs were obtained with stimuli consisting of clicks of 80 �s duration. The stimulus level in the outer ear was set at 80 � 3 dB pe SPL. The click rate was 50 per second and post-stimulus analysis was in the range of 2 to 20 ms. A total of 260 sweeps was averaged above the noise rejection level of 47 dB. Stimuli were presented in the nonlinear mode, in which every fourth click stimulus is inverted and three times greater in amplitude than the three preceding clicks. A transiently-evoked OAE was defined as a response if its amplitude was > 3 dB above the level of the noise floor. Reproducibility percentages > 60 percent was taken into account as acceptable for the analysis at five successive frequency bands from 1 to 5 kHz.
Distortion-product OAEs were measured as DPgram, where the intensity levels of the primary tones are held constant and distortion-product OAE data are recorded for different frequency regions, from 1 to 6.3 kHz and plotted as a function of f2. The resolution of DPgram recording was obtained at four points per octave. The frequency ratio of the two primary tones (f2/f1) was fixed at 1.22. Stimulus levels were kept at 65 dB for f1 and 55 dB for f2 frequencies. Distortion-product OAE measurement at 2f1-f2 was considered significantly different from the background noise if it exceeded by at least 3 dB.
Results
Since all our subjects had normal hearing, the transiently-evoked OAEs were recorded above the noise floor from 1 to 4 kHz, but below the noise floor at 5 kHz. Similarly, the reproducibility percentages were above 60 percent for 1 to 4 kHz and below for 5 kHz. In the DPgram, the emission amplitude levels were greater than the noise floor throughout the testing frequencies from 1 to 6.3 kHz for all sessions. The first and second measurements were not significantly different, demonstrating the high repeatability of the evoked OAEs. There was no statistically significant difference in the mean amplitudes of the evoked OAEs between the second (before the EMF exposure) and third (after the EMF exposure) measurements, in addition to the four separate testing measures (p > 0.05).
The results of this study suggest that 10-minute EMF exposure from the mobile telephone did not cause any detectable alteration on evoked OAE measurements. Since there was no significant difference between the testing session, the last testing for the purpose of recovery of the potential hearing effect had been in vain. Figure 1 and 2 graphically depict the average amplitude levels of the transiently-evoked and distortion-product OAEs, respectively.
 Figure 1 Figure 1: Mean amplitudes and reproducibility percentages of the transiently-evoked OAEs with standard deviations, and mean noise floor levels with standard deviations in four sessions of measurements 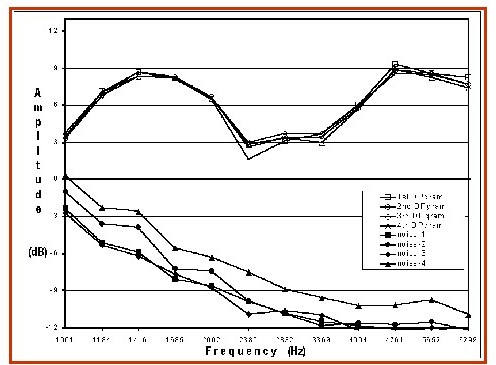 Figure 2 Figure 2: Mean amplitudes of the distortion-product OAEs and noise floor levels in four sessions of measurements
Discussion
A rapid worldwide expansion of mobile telephones raises questions regarding possible effects of the emitted radiofrequencies on the health of the consumers. Of all anatomical structures, the ear has one of the closest proximity to mobile telephones. This may lead to relatively high SAR deposition in the ear compared to other parts of the body. Although the effect of mobile telephones on hearing aids was studied, there is no investigation on hearing itself. After confirming the test-retest reliability, the outcomes of this study were based on the comparison of evoked OAE parameters prior to and following exposure to the EMF. This exposure was achieved by having subjects hold the activated mobile telephone for 10 minutes without conversation and interruption for the purpose of being exposed to EMF per se.
Under certain stimulus conditions, the healthy cochlea emits acoustic energy that is objectively measurable in the ear canal. Monitoring the status of the outer hair cell, the most vulnerable structure of the cochlea, has been shown to provide a very sensitive index of cochlear damage. Mild cochlear functional changes, not revealed in pure-tone audiometry, cause obvious changes in distortion-product OAEs. Evoked OAEs are also a well-described method for detecting the effects of ototoxic drugs on the cochlea. The high test-retest reliability of OAE measures permits the utilization of these emissions to monitor dynamic changes in cochlear responsiveness.
The measurement of the evoked OAEs is non-invasive, painless and quick and it does not require active participation of individuals. For these reasons, OAE measurements appeared to be well suited for the investigation of potential cochlear involvement from the exposure of the mobile telephone EMF.No input/output functions were recorded because of the necessity to minimize the test duration following the EMF exposure not to miss the temporary threshold changes.
Alternative methods, such as pure tone audiometry and Békesy audiometry were not utilized for the evaluation of the possible effects of mobile phone EMF on hearing. Because they are subjective, protracted and, less sensitive methods for subtle cochlear involvements. Both the transiently evoked and distortion-product OAEs have a great potential in the detection of temporary threshold shifts after cochlear insults. Transiently evoked OAEs provide a more sensitive and more objective method of detecting a subtle noise-induced disturbance of cochlear function than do pure tone audiometry or distortion-product OAEs, and it is measured in a shorter time than the DPgram. Hence, we have started testing firstly with transiently evoked OAEs and, DPgram followed immediately after.
The only potential insult to which the subjects were exposed during in this investigation was a 10-minute use of the mobile telephone. Transiently-evoked OAEs were analyzed in terms of emission level and reproducibility as a function of frequency (1 to 4 kHz). These parameters recorded at 5 kHz were not valid for evaluation. Distortion-product OAEs were obtained as DPgrams from 1 to 6.3 kHz. The DPgram amplitudes were determined for each subject. Since transiently evoked OAEs are practically most reliable between 1000 and 4000 Hz and distortion-product OAEs between 2000 and 6000 Hz, both types of evoked OAEs were utilized to take advantage of their differing frequency sensitivity. Four consecutive measurement sesions did not demonstrate any significant changes in emission amplitudes.
Statistical analyses of the evoked OAE levels among testing sessions, corroborate that mobile telephone use does not cause any after-effect on hearing in neither a positive nor a negative manner. If the mobile telephone use should have caused significant impact on the cochlea, the OAE measurements which are very sensitive even to subtle cochlear alterations, would have suggested so.
Radiofrequency electromagnetic radiation is emitted from mobile telephone's antenna. It can penetrate into the organic tissue and be absorbed and converted into heat. The close proximity of a mobile telephone antenna to the user's ear may lead to the deposition of a large amount of EMF energy to the ear. This energy radiated by a mobile telephone is low. GSM telephones always emit the maximum power for a few seconds during initiation of the connection with the mobile telephone. The telephone rings only after the telephone has received this powerful transmission and the power decreases to the level which is just enough for the connection. This protective feature of the GSM mobile telephones may have a role for the negative results of the study.
The rate of absorption and the distribution of EMF energy in a tissue depends on many factors. These include: the dielectric composition of the irradiated tissue, e.g., the bone having a lower water content absorbs less energy than muscle; the frequency of the EMF; shape, geometry, and orientation of the object; and closeness of the source. Heating of biological tissue can occur as a consequence of EMF energy absorption by the water in the tissue. The rise in temperature depends primarily on the intensity of the radiation and the efficiency of the thermoregulation mechanism of the body. In deep tissues, like the brain, maximum temperature rise due to mobile telephone EMF exposure was calculated to be no more than about 0.1o C. This is similar to the normal daily fluctuations in body temperature and is considered to be too low to cause adverse effects. It is speculated that since the cochlea is enclosed by very dense compact bone, located relatively deep and congested with the perilymph and endolymph, it is realtively shielded from the EMF radiation generated by the mobile phone.
The results of the present study may appear comforting for the safety of mobile telephones on hearing. But it is not sufficient to conclude that exposure to EMF during the use of mobile telephones do not lead to any hazardous health effects. Since the electromagnetic emissions from the mobile telephone would interfere with the detection and recording of the emission apparatus, hearing could not be evaluated simultaneously with mobile telephone use, but only instantly following the EMF exposure. Therefore, the status of the cochlea during mobile telephone use is still obscure. Unfortunately, the cost of mobile telephone utilization greater than 10 minutes for each volunteer was financially prohibitive in the study. Even so, an average individual usually speaks on the mobile phone less than 10 minutes for each occasion in our daily life.
To the best of our knowledge this was the first study evaluating the hearing effects of mobile telephones EMF. A-ten minute close exposure to EMF emitting from a mobile telephone had no after-effect on hearing, at least the non-linearity of the outer hair cell functions was not altered. This study was designed for a short time acute exposure and the results gained do not reveal any information regarding the potential effects of longer airtime or chronic cumulative exposure. Thus, it is recommended that further studies examine whether hearing would be affected after longer or repeated EMF exposures.Since little is known about the biological effects of mobile telephone use, there are scientific gaps and suspicions that the EMF radiating from the mobile telephones can have detrimental health results. Therefore, the following prudent use of mobile telephones is recommended: use mobile telephones for as short of periods as possible, only for essential purposes, with low SAR values and with hands-free devices provided that they have been proved to reduce SAR exposure References
Szentpali B. Human exposure to electromagnetic fields from mobile phones. IEEE 1999; 222-31.
Frey AH. Headaches from cellular telephones: are they real and what are the implications? Environ Health Perspect 1998; 106:101-3.
Oftedal G, Wilen J, Sandstrom M, Mild KH. Symptoms experienced in connection with mobile phone use. Occup Med 2000; 50:237-45.
Fritze K, Sommer C, Schmitz B, Mies G, Hossmann KA, Kiessling M, Wiessner C. Effect of global system for mobile communication (GSM) microwave exposure on blood-brain barrier permeability in rat. Acta Neuropathol (Berl) 1997; 94:465-70.
Borbely AA, Huber R, Graf T, Fuchs B, Gallmann E, Achermann P. Pulsed high-frequency electromagnetic field affects human sleep and sleep electroencephalogram. Neurosci Lett 1999; 275:207-10.
Braune S, Wrocklage C, Raczek J, Gailus T, Lucking CH. Resting blood pressure increase during exposure to a radio-frequency electromagnetic field. Lancet 1998; 351:1857-8.
Preece AW, Iwi G, Davies-Smith A, Wesnes K, Butler S, Lim E, Varey A. Effect of a 915-MHz simulated mobile phone signal on cognitive function in man. Int J Radiat Biol 1999; 75:447-56.
Repacholi MH, Basten A, Gebski V, Noonan D, Finnie J, Harris AW. Lymphomas in E mu-Pim1 transgenic mice exposed to pulsed 900 MHz electromagnetic fields. Radiat Res. 1997; 147:631-40.
Moulder JE, Erdreich LS, Malyapa RS, Merritt J, Pickard WF, Vijayalaxmi. Cell phones and cancer: what is the evidence for a connection? Radiat Res 1999; 151:513-31.
International Non-Ionizing Radiation Committee of the International Radiation Protection Association. Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic field (up to 300 GHz). Health Phys 1998; 74:404-522.
Hyland GJ. Physics and biology of mobile telephony. Lancet 2000; 356:1833-36.Byrne D, Burwood E. The Australian experience: global system for mobile communications wireless telephones and hearing aids. J Am Acad Audiol 2001; 12:315-21.
Kemp DT. Development in cochlear mechanics and techniques for noninvasive evaluation. Adv Audiol 1988; 5:27-45.
Ozturan O, Jerger J, Lew H, Lynch GR. Monitoring of cisplatin ototoxicity by distortion-product otoacoustic emissions. Auris Nasus Larynx (Tokyo) 1996; 23:147-51.
Lonsbury-Martin BL, McCoy MJ, Whitehead ML, Martin GK. Clinical testing of distortion-product otoacoustic emissions. Ear Hear 1993; 14:11-22.
Plinkert PK, Hemmert W, Wagner W, Just K, Zenner HP. Monitoring noise susceptibility: sensitivity of otoacoustic emissions and subjective audiometry. Br J Audiol 1999; 33:367-82.
Vinck BM, Van Cauwenberge PB, Leroy L, Corthals P. Sensitivity of transient evoked and distortion product otoacoustic emissions to the direct effects of noise on the human cochlea. Audiology 1999; 38:44-52.
Hall JW. Handbook of Otoacoustic Emissions. Singular Publishing Group, SanDiego, Calfornia, 2000; pp 354.
Engdahl B, Kemp D. The effect of noise exposure on the details of distortion-product otoacoustic emissions in humans. J Acoust Soc Am 1996; 99:1573-87.
Van Leeuwen GM, Lagendijk JJ, Van Leersum BJ, Zwamborn AP, Hornsleth SN, Kotte AN. Calculation of change in brain temperatures due to exposure to a mobile phone. Phys Med Biol 1999; 44:2367-79.
|




